szept. 30, 2022 by Philips
Reading time: 4-5 minutes
Learn how St. Antonius Hospital reduced non-actionable ICU alarms by 40%

In every intensive care unit (ICU), medical device alarms serve a critical role in patient care and safety by alerting staff to important information about patient health and equipment function. However, studies show that only 5-13 percent of alarms are clinically relevant.*1 The high sensitivity and low specificity of alarms has unintended consequences: the cacophony of beeping is not conducive to patient rest or a low-stress environment, and it can induce alarm fatigue, in which staff becomes desensitized to alarms, which compromises patient safety. The conundrum for ICUs everywhere is how to reduce unnecessary alarms without sacrificing those that are essential to patient care. St. Antonius Hospital (Nieuwegein, The Netherlands) set an ambitious goal: a 30% reduction in the number of alarms per bed per day in the ICU, without any impact on quality of care.
Improving patient care and staff satisfaction by reducing ICU alarms
Learn more about St. Antonius Hospital’s successful approach to reducing irrelevant ICU alarms.
Step one: choose monitors that support alarm management goals
One of the first steps that the hospital took towards more effective alarm management was equipping its ICU with Philips IntelliVue patient monitoring systems. IntelliVue monitors offer a number of advanced algorithms and features designed to give healthcare facilities more flexibility in setting up and managing alarms. Features such as Smart Alarm delay SpO2, flush/blood sample detection in the invasive blood pressure measurement, and automatic alarm limit adjustment help reduce non-actionable alarms. Different alarm profiles can also be created for specific patient groups for added flexibility.
Step two: measure
Understanding that choosing effective monitors is only part of the solution, the team at St. Antonius asked Philips Clinical Services to help them reach their goal. Philips consultants began by interviewing stakeholders, including nurses, physicians and others, to evaluate the impact of alarming. Next, they measured the number of alarms generated by bedside monitors in the ICU to establish a baseline for the project.
Objective data is key
Data was the critical factor throughout the process, according to Ineke van de Pol, project champion and ICU nurse practitioner. “Every root cause we looked at, every change we made, we validated all of it with actual data,” she says. “That allowed us to see the impact of what we were doing. Without that data, we could never have done this. That was a big advantage of working with Philips because they could easily collect this data for us. They knew how to read the numbers and we could then make decisions about what steps to take.”
Every root cause we looked at, every change we made, we validated all of it with actual data.”
Ineke van de Pol
Project champion and ICU nurse practitioner
The results of the measurements surprised even those who had commissioned the project. On average, 344 alarms per bed went off every day in the St. Antonius ICU. That translates to one alarm every 3-4 minutes! The consultants also measured the number of alarms that were ignored. Dr. Wirds says, “I was really surprised by the number of alarms that went off, but where no action was taken. Then you realize that a certain percentage of alarms provide no added value to your clinical process.”
Van de Pol says, “When we heard those numbers, we were all shocked. No one expected it to be so high. It was a very motivational moment for the entire team when you saw what the actual numbers were.”
“I think that many people who work with monitors all day have no idea what they can do with the data they have,” says Dr. J.W. Wirds, anesthesiologist. “There is so much information available, but we really needed the help of the consultants at Philips who knew how to analyze the data and could help us see how to use the technology to improve our care environment.”
Step three: identify causes and enact solutions
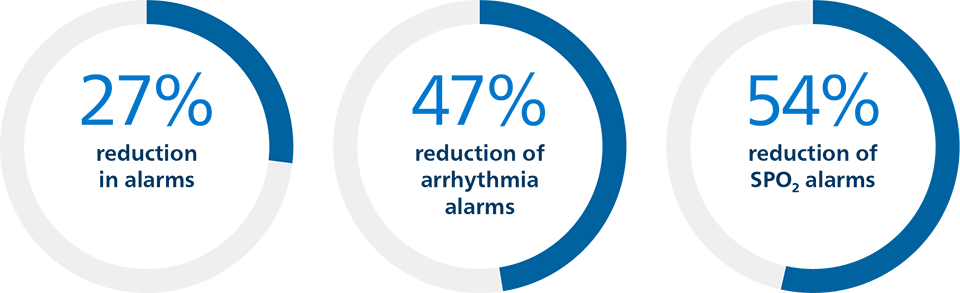
The team immediately identified where clinically irrelevant changes in patient data were triggering unnecessary alarms. For example, the monitors were set to alarm when a patient’s heart rate exceeded 110 beats per minute (bpm). The data showed that many patients’ heart rates would reach 111 bpm, triggering an alarm. “This was not life-threatening, and by re-setting the alarm threshold to 115 we greatly reduced a number of unnecessary alarms without affecting the quality of care,” says Dr. Wirds. The staff also committed to turning off patient monitors during procedures, such as drawing blood. Prior to this directive, the monitors were left on two-thirds of the time, which triggered unnecessary alarms. These phase one initiatives resulted in a 27% reduction in alarms, from 344 to 249 alarms per bed per day. Arrhythmia alarms were reduced by 47% and SPO2 alarms were reduced by 54%.
Education is also critical to reducing alarms, and the team focused on this during the second phase of the project, training super users and making alarm education a standard module in ICU nurse training.
In addition, the hospital instituted a second alarm profile for medium-care patients, rather than using the same parameters for all patients. This profile further reduced clinically irrelevant alarms.

Final result: 40% alarm reduction
“After all the changes we made, we reduced our alarms by 40% – exceeding our initial goal by a quarter,” says van de Pol. “We are now down to 204 alarms per bed per day. It’s much quieter now. There is much less noise and we have a more pleasant work environment.”
One important advantage is that the staff now know that the alarms they do hear are relevant. They know they need to pay attention to them.”
Dr. J. W. Wirds
Anesthesiologist
“This whole process raised our consciousness about the importance of alarm management,” Van de Pol says. When you are working around these signals all day long, you tend to accept it as normal. We all thought that the alarms weren’t such a big issue. We didn’t realize just how big the problem was or how much better we could make the situation.”
*The definitions of clinical relevance were inconsistent across the studies included in the literature review.
Takeaways
*2021 Patient Safety Goal can be found at: https://www.jointcommission.org/-/media/tjc/documents/standards/national-patient-safety-goals/2021/npsg_chapter_hap_jan2021.pdf
1 Ruppel H, Funk M, Whittemore R. Measurement of Physiological Monitor Alarm Accuracy and Clinical Relevance in Intensive Care Units. Am J Crit Care (2018) 27 (1): 11–21.
Explore our acute patient management products and capabilities
Share this case study
Sign up to receive news and updates from Philips.
At a glance Challenge Solution Results 40% reduction in non-actionable ICU alarms
St. Antonius Hospital ICU Department
Nieuwegein, The Netherlands
Reduce the number of irrelevant ICU alarms in a new ICU facility
Philips IntelliVue patient monitoring systems and Philips Clinical Services
Explore more
-
![Saratoga Hospital reduces patient transfers from orthopedic unit to the ICU by 63%]()
Saratoga Hospital reduces patient transfers from orthopedic unit to the ICU by 63%
Read the story -
![Enhancing patient outcomes, hospital flow and resource utilization through timely care transitions in the ICU]()
Enhancing patient outcomes, hospital flow and resource utilization through timely care transitions in the ICU
Read the story

